

What Are The Stages Of Fracture Repair
Introduction [edit | edit source]
Bone fractures is a common injury and the healing procedure is complex.[1] Bone is ane of a few tissues that are able to heal without forming a gristly scar. There are two types of fracture healing – indirect (secondary) and direct healing (primary).[two]

Fracture of 4th Metacarpal Bone
Direct/ primary healing occurs when the bony fragments are fixed together with compression. There is no callus formation. The bony ends are joined and healed by osteoclast and osteoblast activity. [1]
Indirect healing is more common than direct healing and involves both endochondral and intramembranous bone healing.[2] Anatomical reduction and stable atmospheric condition are not required for indirect healing to occur.[2] Rather, there is a minor amount of motion and weight-bearing at the fracture, which causes a soft callus to form, leading on to secondary bone formation.[1] Information technology should exist noted though that too much load/motion tin can consequence in delayed healing or not-union,[ii] which occurs in 5-10% of all fractures.[three]
Indirect healing usually occurs with:
- Not-operative fracture treatment
- Operative treatments where some motion occurs at the fracture site, such as:
- Intramedullary nailing
- External fixation
- Internal fixation of comminuted fractures.[2]
Stages of Indirect Healing [edit | edit source]
Acute Inflammatory Response [edit | edit source]
The astute inflammatory response peaks inside 24 hours and ends after vii days and is essential for healing to occur.[two] A haematoma forms immediately after trauma. This consists of cells from the peripheral and intramedullary blood and os marrow cells. The inflammatory response causes the haematoma to coagulate effectually the fracture ends and within the medulla, which creates a model for callus formation.[2]
Tumor necrosis factors TNF-α, interleukin-1,IL-half-dozen, IL-11, and IL-xviii are releases to maintain and promote blood vessels growth[4].
Recruitment of Mesenchymal Stem Cells [edit | edit source]
Bone is unable to regenerate unless specific mesenchymal stalk cells are recruited, proliferated, and differentiated into osteogenic cells. It is not currently understood exactly where these cells come from.[2]
Generation of Cartilaginous and Periosteal Bony Callus [edit | edit source]
After the hematoma has formed, a fibrin-rich granulation tissue forms. Endochondral formation occurs between the fracture ends and across the periosteal sites in this tissue. These areas are less stable, so the cartilaginous tissue forms a soft callus, giving the fracture more stability.[2]
In animal studies, soft callus formation peaks at 7 to 9 days when type Ii procollagen and proteoglycan cadre protein extracellular markers are at their highest levels.[2] Meantime, an intramembranous ossification response occurs subperiosteal immediately by the fracture ends. This creates a difficult callus. The bridging of this fundamental hard callus provides the fracture with a semi-rigid construction which enables weight-bearing.[2]
Revascularization and Neoangiogenesis [edit | edit source]
Adequate blood supply is necessary for bone repair to occur. Angiogenic pathways, chondrocyte apoptosis, and cartilaginous deposition are essential to this procedure because cells and extracellular matrices must be removed in social club to ensure that blood vessels tin can move into the repair site.[2]
Mineralization and Resorption of the Cartilaginous Callus [edit | edit source]
![]()
Healing with callus formation
The chief soft cartilaginous callus must be resorbed and replaced by a difficult bony callus for bone regeneration to go on.[two] In some ways, this stage repeats embryological os evolution and involves cellular proliferation and differentiation, every bit well as an increase in cellular book and matrix deposition.[2]
Os Remodeling [edit | edit source]
While the hard callus is rigid and provides stability, it does not mean that the fracture site has all the properties of normal os. A 2d restorative stage is necessary. This stage results in the remodeling of the hard callus into a lamellar bone construction with a central medullary cavity.[2]
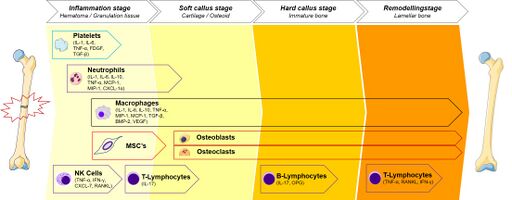
Remodeling occurs when the difficult callus is resorbed by osteoclasts and lamellar os is deposited by osteoblasts. This starts at 3–4 weeks, simply the whole procedure may accept years. Remodeling may be faster in younger patients (and other animals).[2]
Bone remodeling results from the product of electrical polarity. This occurs when force per unit area is applied in a crystalline environment.[2]
- When centric loading of long bones occurs, an electropositive convex surface and an electronegative concave surface are created
- This activates osteoclastic and osteoblastic activity.
- As a event, the external callus is slowly replaced by a lamellar os structure. Equally well equally this, the internal callus remodels which re-creates a medullar crenel, like to diaphyseal bone.[2]
Bone remodeling will only exist successful if there is adequate claret supply and a gradual increase in mechanical stability. If not, complications such as non-union may occur.[2]
Direct Fracture Healing [edit | edit source]
Straight healing requires reduction of the fracture ends, without whatsoever gap formation, every bit well as stable fixation. Thus, it does not normally occur naturally only rather post-obit open reduction and internal fixation surgery.[ii]
Direct os healing tin can occur by direct remodeling of lamellar bone, the Haversian canals, and blood vessels. The process usually takes from months to years.[2]
Principal healing of fractures occurs through:
- Contact healing
- Gap healing.
Both processes consist of an endeavour to copy lamellar os structure. Direct os healing is possible only when the fracture ends are compressed together and rigid fixation is used to decrease interfragmentary strain.[2] [i]
Contact Healing [edit | edit source]
A fracture can unite by contact healing when the gap betwixt each bone finish is less than 0.01 mm and interfragmentary strain is less than 2%.[2] In such instances cut cones course at the ends of the osteons by the fracture site. The tips of the cutting cones consist of osteoclasts. These tips cantankerous the fracture line and generate longitudinal cavities.[2]
The cavities are eventually filled by bone that is produced past osteoblasts. This causes the bony wedlock to generate while also restoring the Haversian systems, which are formed in an axial direction. The Haversian systems enable blood vessels carrying osteoblasts to enter the area. Bridging osteons eventually mature into lamellar bone, which results in fracture healing without a periosteal callus forming.[two]
Gap Healing [edit | edit source]
Gap healing is unique in that bony wedlock and Haversian remodeling does non happen at the same time.[2] For gap healing to occur, the gap must exist less than 800 μm to i mm.[2]
During this process, the fracture site is filled largely past lamellar bone which runs perpendicular to the long axis and needs secondary osteonal reconstruction. The primary os construction is eventually replaced by longitudinal revascularized osteons, which carry osteoprogenitor cells that differentiate into osteoblasts. These osteoblasts and so produce lamellar os on each surface of the gap.[two] The lamellar bone is laid down perpendicular to the long centrality, which means that information technology is non strong. This procedure takes betwixt 3 and 8 weeks. Subsequently this, a secondary remodeling phase occurs, which is similar to the pour with cut cones in contact healing.[2]
Factors Touch on Os Healing [edit | edit source]
- Patient with nutritional deficits, smoking, and diabetic patient volition experience delayed bone healing.
- Parathyroid hormones have a vital part in bone healing by stimulating the differentiation and proliferation of osteoblasts and osteoclasts.
- Aging process in which the patient volition have:
- Chronic inflammation or the delay in resolving the inflammation to set for the anabolic process affect healing and cause a small callus formation, in add-on to higher levels of circulating pro-inflammatory cytokines.
- Patient at this age will show a subtract in the quantity of the muscle stem cells and negatively affect impact the healing process.
- Decrease in the bone marrow blood vessels compared to young historic period and decrease in vascularization and angiogenesis[5].
- Factors related to the fracture site:
- Infection of the fracture site at healing process.
- Insufficient formation of cartilage within fracture gap and marrow space.
- Open, comminuted fracture, and the extent of soft tissue injury also show delayed marriage healing[6].
[7]
References [edit | edit source]
- ↑ i.0 1.one one.ii i.three Ghiasi MS, Chen J, Vaziri A, Rodriguez EK, Nazarian A. Bone fracture healing in mechanobiological modeling: A review of principles and methods. Os Rep. 2022; 6: 87-100.
- ↑ 2.00 2.01 2.02 two.03 2.04 two.05 2.06 2.07 2.08 2.09 2.ten 2.11 2.12 2.13 two.fourteen 2.xv two.sixteen 2.17 2.eighteen two.19 ii.twenty 2.21 ii.22 ii.23 2.24 2.25 2.26 2.27 two.28 Marsell R, Einhorn TA. The biology of fracture healing. Injury. 2022; 42(vi): 551-555.
- ↑ Buza JA, Einhorn T, Os healing in 2022. Clin Cases Miner Os Metab. 2022; xiii(2): 101-105.
- ↑ Beckmann R, Tohidnezhad M, Lichte P, Wruck CJ, Year H, Pape HC, Pufe T. From former to new.relevant factors for fracture healing in aging os. The orthopedist. 2022 April; 43 (iv): 298-305.
- ↑ Clark D, Nakamura M, Miclau T, Marcucio R. Effects of aging on fracture healing. Electric current osteoporosis reports. 2022 Dec i;15(6):601-8.
- ↑ Kostenuik P, Mirza FM. Fracture healing physiology and the quest for therapies for delayed healing and nonunion. Periodical of Orthopaedic Research®. 2022 Feb;35(2):213-23.
- ↑ Osmosis. Os remodeling and repair. Available from: http://www.youtube.com/spotter?v=Ei4seya3dOg[concluding accessed viii/8/2021]

What Are The Stages Of Fracture Repair,
Source: https://www.physio-pedia.com/Bone_Healing
Posted by: quandttoofte01.blogspot.com
0 Response to "What Are The Stages Of Fracture Repair"
Post a Comment